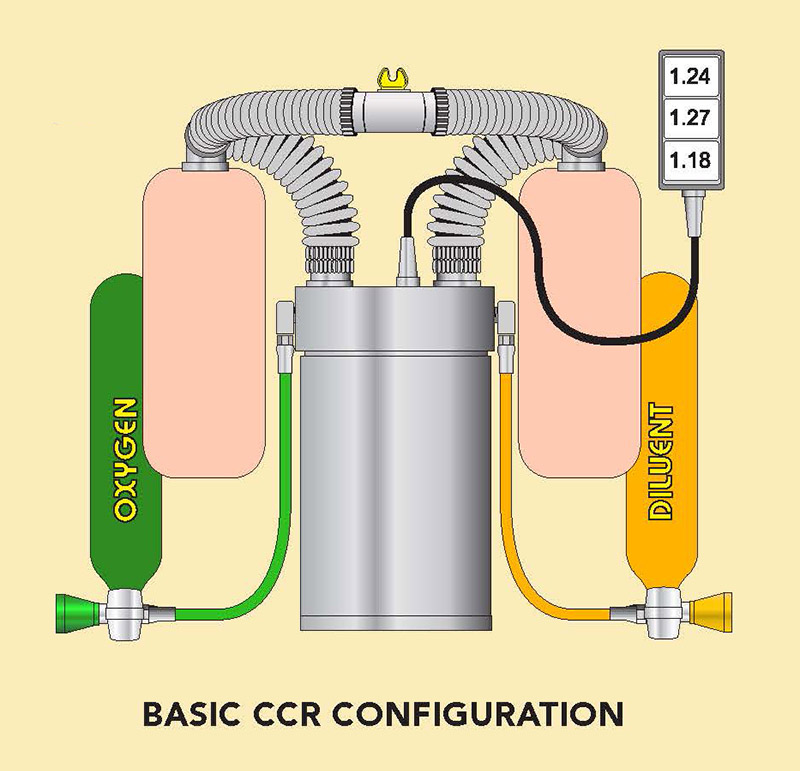
Rebreathers come in all different sizes, shapes, and even colors; but if you were to break them down into the most basic components, they all contain the same fundamental parts. The difference between rebreather models is the manufacturer’s design, and how they have placed these basic parts into their CCR configuration. Other features are merely the bells and whistles added to the manufacturer’s package to complete the same basic tasks of simply adding desired amounts of oxygen, scrubbing out unwanted carbon dioxide, and monitoring gas partial pressures within the system.
The new rebreather diver researches the different models and manufacturers and purchases the unit he/she feels best suits the type of diving that is expected. As most CCR divers gain experience, become comfortable, and move on to more and more demanding dives, the standard rebreather often ceases to provide the diver with the best configuration for the increased dive exposure.
This editorial aims to enlighten divers who have reached this critical stage of rebreather diving and provide alternative CCR configuration ideas that may better suit extended or remote rebreather exposures.
The above graphic illustrates the most basic rebreather design containing the simplest parts that all rebreathers are designed from.
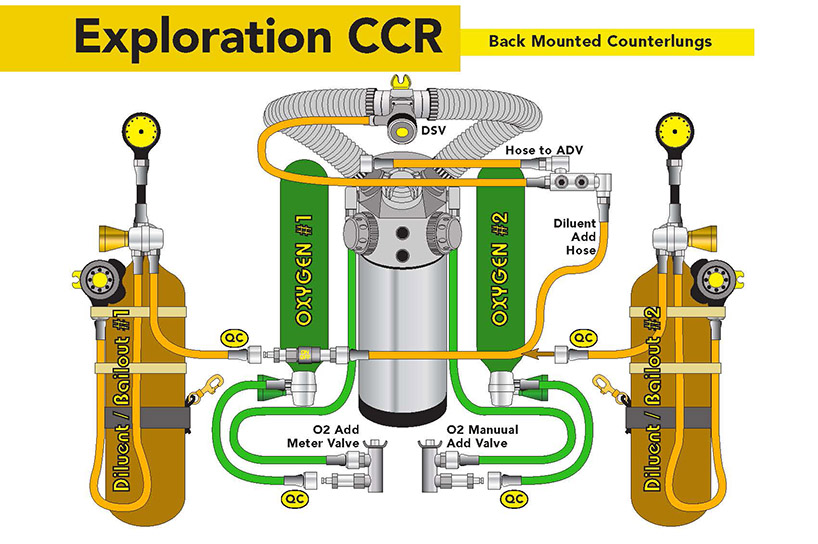
Exploration CCR / Back Mounted Counterlungs (fig 1)
The configuration of the exploration CCR allows the technical explorer to fully utilize the possibilities of extreme depths and long dive durations that the rebreather is designed to provide.
Oxygen: One key ingredient that is needed to make a closed circuit rebreather work is oxygen. Without oxygen, the closed circuit rebreather loses the advantages of maintaining a constant PPO2 to maximize bottom time and minimize decompression times. On a standard rebreather configuration, the unit attaches an oxygen and diluent cylinder, which normally range between 13 and 18 cubic feet each. At extreme depths or lengthy cave / wreck penetrations, this small amount of diluent is essentially worthless in an emergency. On the exploration CCR, the small diluent cylinder is replaced by a second oxygen cylinder that is connected into the loop via a totally separate port than the main oxygen addition valve. This doubles the amount of oxygen carried during a dive and adds a totally redundant oxygen addition method into the rebreather loop. The quick-connect ports allow for easy connection of additional oxygen from off-board stages into the expedition unit at any time.
Diluent: If a failure should occur at any point during a dive, the diver is required to either switch to a semi-closed mode or, in worst-case scenarios, to open circuit. If the diver has planned his/her diluent correctly by selecting a gas mix containing the optimal oxygen percentage at the planned depth, the semi-closed mode will slightly increase the decompression obligations. The major problem with switching to open circuit is the amount of gas required to return safely to the surface, along with the heavily increased decompression obligations that will result from losing the optimal PPO2.
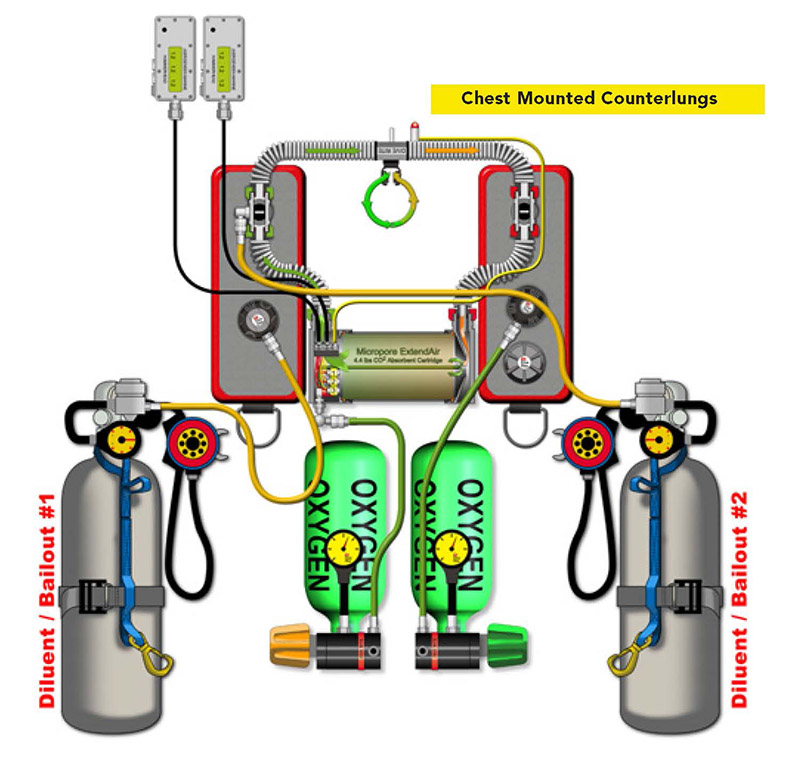
Exploration CCR / Front Mounted Counterlungs (fig 2)
The major difference between the two illustrations above is the location of the rebreather’s counter lungs. The KISS Classic illustration (Fig 1) has back-mounted counter lungs while the Dive Rite O2ptima (Fig 2) contains chest-mounted counter lungs. On the KISS Classic unit, the diver is required to install some extra hoses and fittings to add the second oxygen cylinder and a simple quick-connect hose attached to the rebreather’s gas manifold block for off-board diluent addition. On the O2ptima (as on most chest-mounted counter lung rebreathers), the manufacturer has already added manual oxygen and diluent quick-connect ports onto the chest-mounted counter lungs, making adding off-board gas simple. Both front and back mounted counter lung units work equally well; the only difference is the diver’s preference for the counter lung location.
With the rising airline weight restrictions and added baggage fees, traveling with any-thing more than your underwear has become exceptionally expensive — let alone attempting to pack in a rebreather, dive equipment, and rebreather cylinders with valves.
Like mountain climbers, traveling rebreather divers are required to cut out every pound possible from their baggage in order to just get the basics to the final destination. Typically, the locations we are traveling to have some type of scuba cylinders, be it actual rebreather bottles or, more commonly, 80 cubic foot aluminums. The simplest method to reduce weight in checked baggage is to forego flying with rebreather cylinders, and just use whatever cylinders you can locate at your destination.
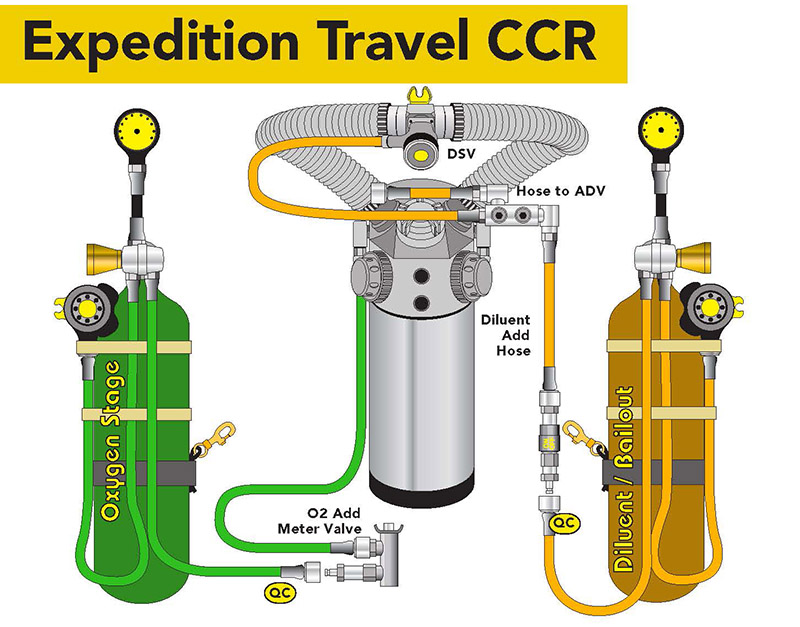
Exploration Travel CCR / (fig 3)
We have termed this rebreather configuration as the expedition travel CCR.
The drawing above illustrates how simple it is to convert a KISS Classic into an expedition travel CCR by simply adding a quick-connect onto the oxygen add valve and a quick-connect hose onto the gas block. (See two images below). Divers can simply quick-connect whatever size cylinders they have attained into the rebreather and side-mount them during the dive.
Chest-mounted counter lung rebreathers such as the Megalodon, CopisMeg, Evolution, and O2ptima are simply converted by adding an oxygen quick-connect to the solenoid injection, and quick-connect into the automatic diluent add valve (ADV). (See two images below.)
One of the other major advantages of the expedition travel CCR is the reduced weight of transporting the unit while at the dive location. Lugging a heavy, equipment-laden rebreather with attached tanks and weights from trucks, onto docks, into rocking boats, or, God forbid, over rocky terrain is extremely difficult and can cause injury.
The expedition travel CCR can be carried easily in one hand or over a shoulder, and handed off without difficulty onto a rocking boat — even without the help of two powerful men and a boy.
CCR Bailout
As stated previously, closed circuit rebreathers provide the diver with the optimal breathing partial pressure of oxygen continuously throughout the dive. This minimizes decompression requirements and maximizes breathing gas conservation.
Another very important factor that most rebreather divers seem to overlook is the heating advantages of closed circuit diving. The warm moist air from exhalation travels through the rebreather and is warmed by the natural heating reaction of the CO2 absorbent material. The diver inhales this heated gas throughout the dive, providing a massive heating advantage that closed circuit cannot.
Without a doubt, rebreathers have bridged the gap into new exploration possibilities that open circuit diving only dreamed of. But with the good can sometimes come the bad.
Equipment Failure
Because of the complexity of many manufactured rebreathers, equipment failure is a high possibility. Depending on what part of the rebreather fails, the diver normally has a list of emergency procedures to fall back on. In most cases, the diver can manage the failure and stay on a closed circuit for the exit. The next option the CCR diver can fall back on is called the semi-closed mode. This is a procedure where the diver can maintain loop integrity by exhaling a percentage of the loop gas into the water and replacing it with fresh, open circuit gas. Even though this procedure does not maintain optimal oxygen partial pressures, it conserves large amounts of gas that would be wasted if the diver had completely switched to open circuit. The last and least desired emergency procedure is for the diver to come completely off the rebreather and go onto 100% open circuit. This procedure loses all the advantages of maximizing decompression, gas conservation, and, many times, the critical thermal protection.
The following tables illustrate the in-creased decompression obligations incurred should a diver be required to bailout onto open circuit from a serious rebreather dive.
CLICK TO ENLARGE CHARTS
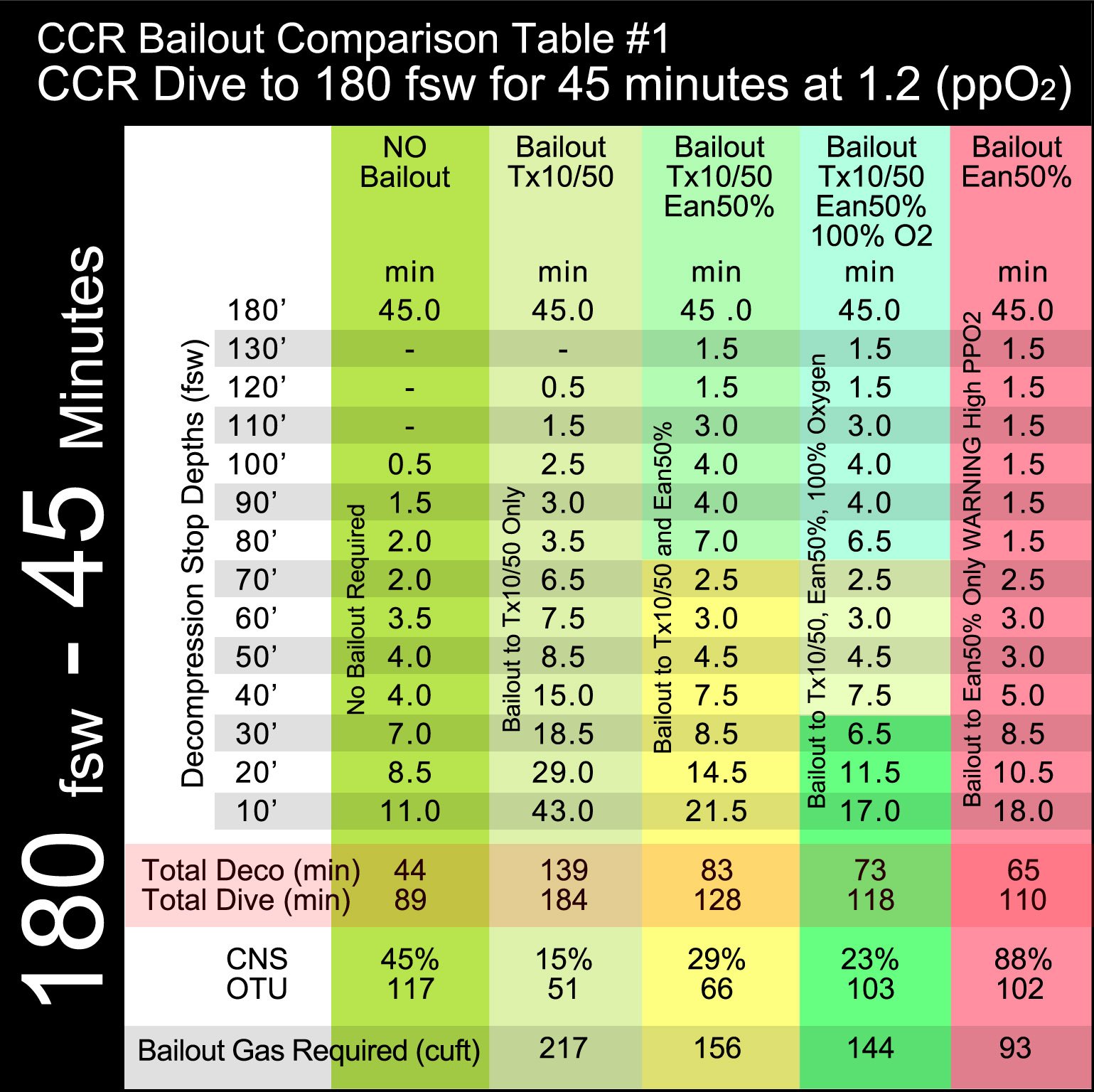
Table 1 above illustrates a closed circuit rebreather dive to 180 feet, maintaining a constant PPO2 of 1.2 for a bottom time of 45 minutes. The left khaki green column calculates the total decompression requirements if the rebreather continued to work properly for a decompression time of 44 minutes, CNS of 45%, OTU of 117, and a total dive time of 89 minutes.
The next column to the right, “Bailout TX 10/ 50,” calculates the increased decompression requirement if the CCR diver is required to bailout to a trimix of 10%O2/50%HE/40%N2 only. Most likely, if the diver had planned his/her emergency gas procedures properly, this would never happen — unless he/she were planning a team bailout and had become separated from the team diver carrying the needed nitrox or oxygen cylinder. Note that the decompression obligation tripled from 44 to 139 minutes. The CNS and OTUs dropped because of the lack of higher oxygen percentages, and the required open circuit gas supply skyrocketed to over 200 cubic feet.
The third column, “Bailout Tx10/50 & Ean50%,” calculates the increased decompression requirement if the CCR diver should be required to bailout to a trimix of 10%O2/50%HE/40%N2 and a 50% nitrox mix. Note the decompression obligation almost doubled from 44 to 83 minutes. The CNS and OTUs rose slightly while the open circuit gas supply remained high at 156 cubic feet.
The fourth column, “Bailout Tx10/50, Ean50% & 100%O2,” calculates the increased decompression requirement if the CCR diver should be required to bailout to a trimix of 10%O2/50%HE/40%N2, a 50% nitrox mix and 100% oxygen. Note the decompression obligation increased from 44 to 73 minutes. The CNS and OTUs rose slightly while the open circuit gas supply remained high at 141 cubic feet.
The last column in pink, “Bailout Ean50%,” illustrates the same dive if the diver were to bailout onto Ean50% only. Note the decompression time was reduced from the “Tx10/50, Ean50% & 100%O2” table, but a high partial pressure of oxygen warning occurred which could increase the risk of oxygen toxicity, resulting in possible convulsions underwater.
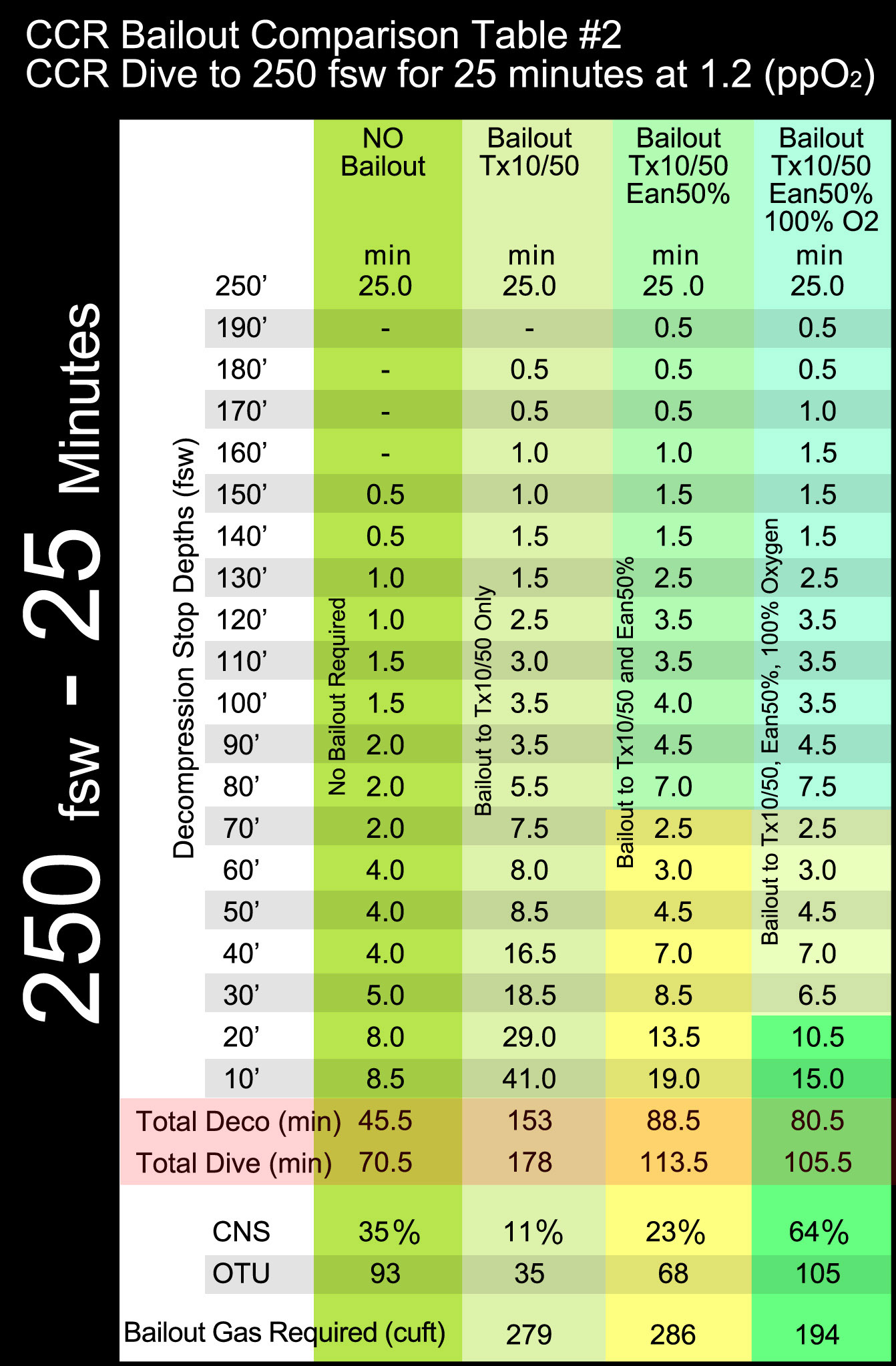
Table 2 above illustrates a closed circuit rebreather dive to 250 feet, maintaining a constant PPO2 of 1.2 for a bottom time of 25 minutes. The columns depict the same gas decompression mixtures as Table 1, illustrating the extreme increase of decompression obligations should the diver be forced to switch onto open circuit. Note the decompression time obligation increases from 45 minutes to 153, 89, and 80 minutes.
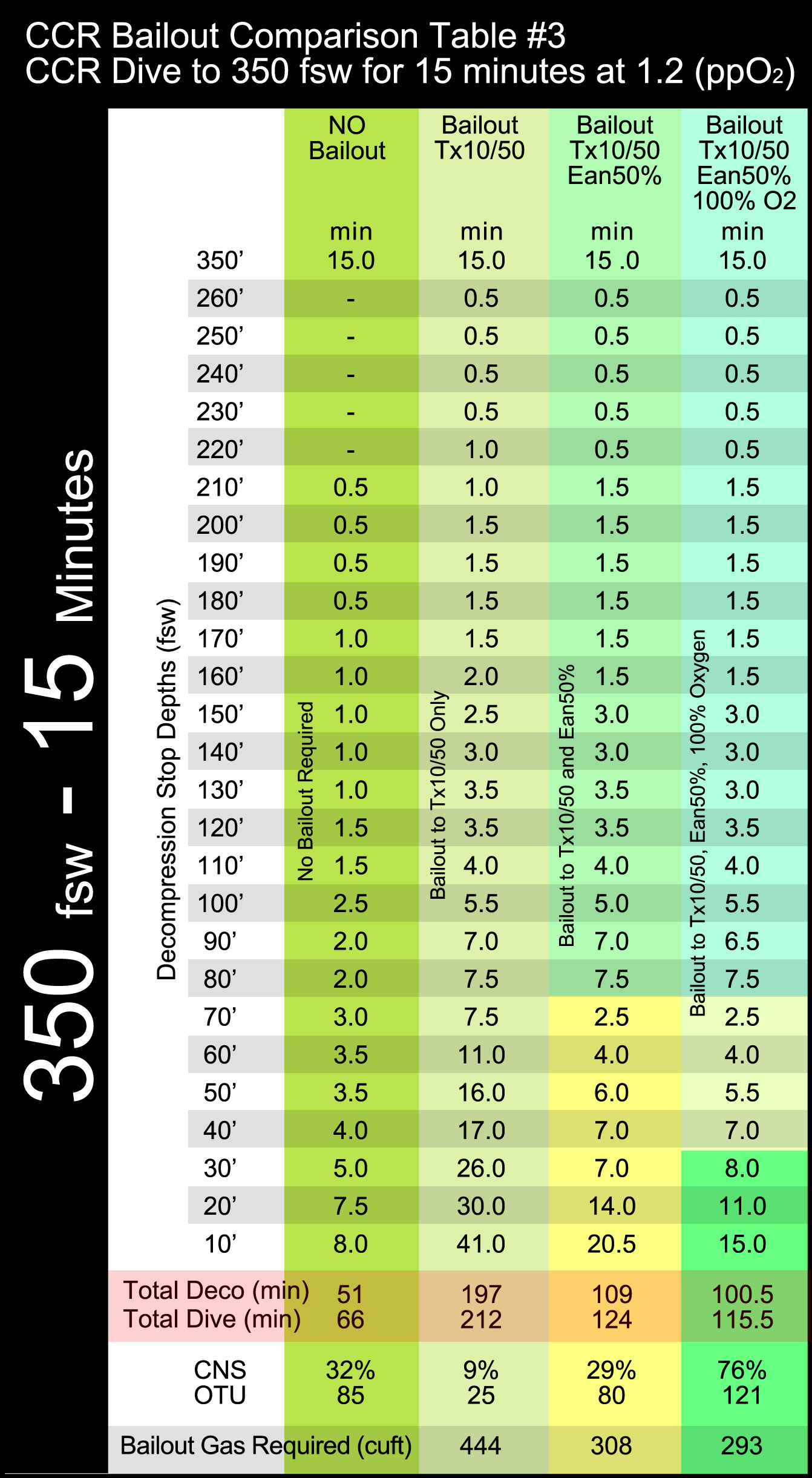
Table 3 above illustrates an extreme closed circuit rebreather dive to 350 feet, maintaining a constant PPO2 of 1.2 for a bottom time of 15 minutes. The columns depict the same gas decompression mixtures as Table 1, illustrating the extreme increase of decompression obligations should the diver be forced to switch onto open circuit. Note the decompression time obligation increases from 51 minutes to 197, 109, and 100 minutes. The open circuit gas supply requirements basically become unmanageable.
Thermal Considerations
Reviewing the increased decompression obligation of the previous three tables clearly illustrates that even if it were possible to supply the increased open circuit gas quantities required, the increased extreme thermal exposures could become more than humanly possible to overcome. A CCR diver wearing a drysuit in 55 degree Fahrenheit water can easily maintain body heat for the simple exposure dive of 250 feet for 70 minutes. However, if we were to lose the increased thermal advantages of the closed loop and increase decompression times to over 170 minutes, in extreme cold conditions, it is doubtful that any human could survive the added exposure.